
Acne vulgaris and its consequent scarring is a long-term process the management of which must be individualized to each case. The age and gender of the person, the severity and extent of acne, the efficacy and tolerability of prior therapies, and the degree of patient’s compliance with the recommended regimen are some of the relevant factors influencing treatment.
The follow-up phase of acne management thus requires a framework for approaching treatment modification that may include concepts such as non pharmacological interventions with various modalities to improve efficacy and tolerability and optimize the outcome while managing acne and scars.
Non pharmacological interventions for acne vulgaris have existed for many years but recently there has been a lot of rise in demand for interventions and with the advent of newer concepts in peels and advances newer avenues have opened up for treating acne and scars.
The medical treatment do have its limitations and though severe acne can be drastically reduced with the best medical therapy, resistant and residual acne still poses a great challenge to dermatologists. Recently newer scar studies have shown that prevention and anti scar treatment have to be initiated in a number of cases while patient is on anti acne regimen or immediately after the acne resolves. The ability of a person to scar after acne depends on patient’s inflammatory profile while healing.
Treating early will help in preventing the progressive scarring of the healing lesions in inflammatory acne.
Chemical Peels
In this era where lasers, lights and energy sources rule the therapeutic interventions, the chemical peels still hold their place firmly as the most widely conducted procedure in our practice.
The technology of graded chemical exfoliation to improve a variety of skin conditions has evolved over years. Today a number of peeling agents are available to us in a wide and bewildering cocktail of formulations. Peels are generally meant to target acne, acne scars, pigmentary conditions, wrinkles and textural improvements that the patients seek. See table 1
Standard and traditional peels have their advantages but are limited by multiple numbers of sittings and inadequate results as perceived by the patients and physicians alike. Limitations of only glycolic peels are inability to use high strength free acid peels as the potential risk of complication increases on Indian pigmented skin and inefficacy of the low strength peels
The basic concept of how the peeling agents work at the tissue level has evolved. Complexities of formulations, molecular size, combinations, mechanism of action, compatibility issues for each peel demands consideration while choosing an appropriate peeling agent which would work best for an indication
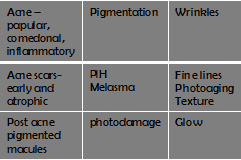
Table 1: Popular peel indications
Based on the new dimension of peel actions, the single agent peels used in the initial years have now paved path for combination of many agents in the same formulation and these combination peels dominate the scene right now. An in-depth knowledge of the dominant molecule in a peel helps one to stay abreast and perform peels with superior results.
Peels are introduced at early stages of anti-acne therapy as they;
- Improve coexisting comedonal and papular acne.
- Alleviate post acne erythema.
- Improve pigmentation at base of healed lesions.
- Improve the depth, contour and cause softening of associated scars.
- Added improvement in texture – glow.
- More youthful appearance of the skin.
Though the alpha, beta hydroxy acids and Trichloroacetic acid (TCA) form the basic peels, we know interplay between these agents is possible and this concept has laid base for development of sound, rational and evidence based revolutionary techniques in peels. The segmental, sequential, rotational, and switch peels are the newer techniques used.
Current trends to optimize outcomes in chemical peels for patient with acne and scars are:
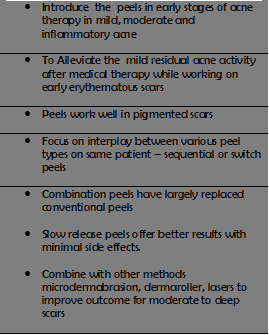
Table 2
A decision to use a peeling agent as an intervention should be made after thorough priming in a well sun protected, compliant patient who has realistic expectations. The priming agents for different indications do differ and this should be taken into account while prescribing.
Indications need to be carefully selected; an acne patient needs a different peel than an early acne scar patient. For acne patients the stage at which a peel is introduced is very essential. Choice of peel is also based on predominance of acne lesions such as comedonal, papular, inflammatory etc. A younger skin responds well to a different formulation than a mature aging skin and pigmentation and texture issues have to be kept in mind at all times while evaluating the outcomes.
Choosing Peels
Combination Peels: Using multiple peeling agents in combinations to compliment their synergistic activity is a recent trend and paved way to newer concepts in peels. The depth and the efficacy of the peels are enhanced with combinations. E.g. a salicylic acid peel combined with a mandelic acid targets the seborrhea, residual acne; post acne pigmented early grade 1 scars as well as textural improvement. The mandelic acid has antibacterial properties and is safer for dark skin types. Gel based combination peels have lesser free acid availability and hence lower incidence of side effects allows one to work safely for sensitive skin types.
Sequential Peels: Peels when used sequentially have the beneficial synergistic actions when compatible agents are chosen. Common technique is one peel is painted and terminated and followed sequentially by another peel in the same sitting which can be terminated or left on slow release peel. Best sequential peels are salicylic acid followed by mandelic acid, a glycolic acid or a retinol peel. Salicylic acid peel or a glycolic acid peel followed by a TCA is another good sequential peel to obtain moderate depth effects.
Switch Peels: Include usage of different peeling agents in rotation in subsequent sittings. One can change peels in subsequent sittings to target the desired problem. E.g. a salicylic acid or a retinol peel in comedogenic or inflammatory acne switched over after clearance to glycolic, mandelic or phytic peels in subsequent sessions to improve scars and texture.
Slow Release Peels
Some of the peels works on the new controlled release principle and are termed as the slow release peels. In these peels a gradual release of the product happens progressively and ensures complete penetration and full action of all components in the solution. The popular Easy phytic peel is composed of three hydroxyl acids with phytic acid, 3 AHA’s are glycolic acid, lactic acid and mandelic acid- the release and action of each is progressive and hence this peel does not need to be ‘Neutralized’ by the physician.
The 3 AHA’s have different rates of penetration in the epidermis, the phytic acid in the easy phytic solution is a large inositol hexaphosphoric acid which fights & neutralizes free radicals, the peeling promotes cell regeneration but during this process it also releases damaging free radicals Phytic acid reduces the cell degeneration induced by free radicals. NO FROSTING should appear-in case of accidental frosting (this may happen if retinol or exfoliating agents have been used) .A sheer vigilance is mandatory as for any other peels. The phytic peel works well for acne residual lesions with early erythematous or pigmented scars of grade 1 or 2. The glycolic acid in the peel works on regeneration and mandelic works on antibacterial and anti-inflammatory properties whereas lactic acid acts as a hydrant and rejuvenating base.
TCA
The trichloreoacetic acid peels are very crucial in improving most types of scars. Depth of the peel can be controlled and generally 15 – 25% strength peels in 4 sessions with adequate priming are very helpful in shallow and rolling boxcar type of scars.
Cross technique: A technique consisting of the focal application of higher trichloroacetic acid (TCA) 40% to 65% concentrations by pressing hard on the entire depressed area of atrophic acne scars. This technique is called chemical reconstruction of skin scars (CROSS).
- Performed for fibrotic and superficial as well as deep
ice pick scars deep rolling and boxcar scars and shows an excellent improvement
in 3 to 5 sittings conducted at monthly intervals. - Repeated CROSS application destroys the atrophic pit
with restructuring and thickening of dermal collagen. - Best results are seen for fibrotic,
ice pick, boxcar scars and dilated pores
CROSS method with dermaroller technique is another way to target improvement in most scars of grade 2 to 3. Cross technique is performed first and in the same sitting followed by a dermaroller therapy in a cycle of 4 to 5 sessions at monthly intervals.
No skin intervention is sans adverse effects and complications.see table 3. Sheer vigilance is of utmost value during peel procedure as most of the adverse effects result from poor priming, noncompliance, wrong peeling agent, etc. Treating skin of color demands additional consideration as one has to focus on preventing pigmentary altercations, so adequate priming and achieving right depth of peel is essential. This is simply achieved by getting the right end point of the peel.
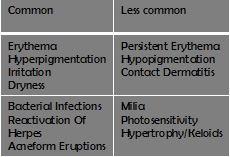
Table 3. Complications of Peels
The beneficial fact is that chemical peels can be combined easily with other procedures like comedone extraction, microdermabrasion, subcision, dermaroller, fractional lasers and skin tightening sequentially for better results
Combination of peels with other Techniques
Application of a salicylic acid peel 20 -30 % or 30 -50% TCA post extraction is helpful not only in alleviation of retinoid resistant comedones but also prevention of recurrence and inflammation. Addition of an oral and a topical antibiotic post extraction prevents pustular flare.
Better results are obtained by combination of microdermabrasion with chemical peels as it helps enhance absorption and uniform penetration of the peeling agent. Microdermabrasion should proceed a week before the chemical peels. Microdermabrasion before phytic peels which are slow release glycolic peels and TCA peels are to be avoided due to potential risk of deeper inadvertent peel absorption and post inflammatory pigmentary changes which is a problem often encountered while dealing with the skin of color.
Microdermabrasion a week before peels, dermaroller after peels, and comedone extraction before salicylic acid or retinol peels can be combined to achieve good results. Fractionated lasers or fillers can be done following the peels after complete reepithelization occurs and inflammation subsides. However emphasis lays on the physician’s clinical acumen to choose an appropriate patient whose clinical condition seems conducive to such combinations.
Conclusion
With multiple treatment options in conjunction with anti acne medical therapy almost all types of difficult acne and mild scars can be alleviated. Early introduction of treatment modalities prevent progressive scarring in inflammatory acne patients. Choosing appropriate treatment options and combining various techniques are individualized from patient to patient and the onus lies on the physician to choose the safest, efficacious, economical method for alleviating the acne and improving the acne scars.
Dislaimer
The information in this article reflects the views of the author only. a qualified health care professional should be consulted before using any therapeutic product discussed. all readers should verify all information and data before treating patients or utilizing any therapies noted in this programme.